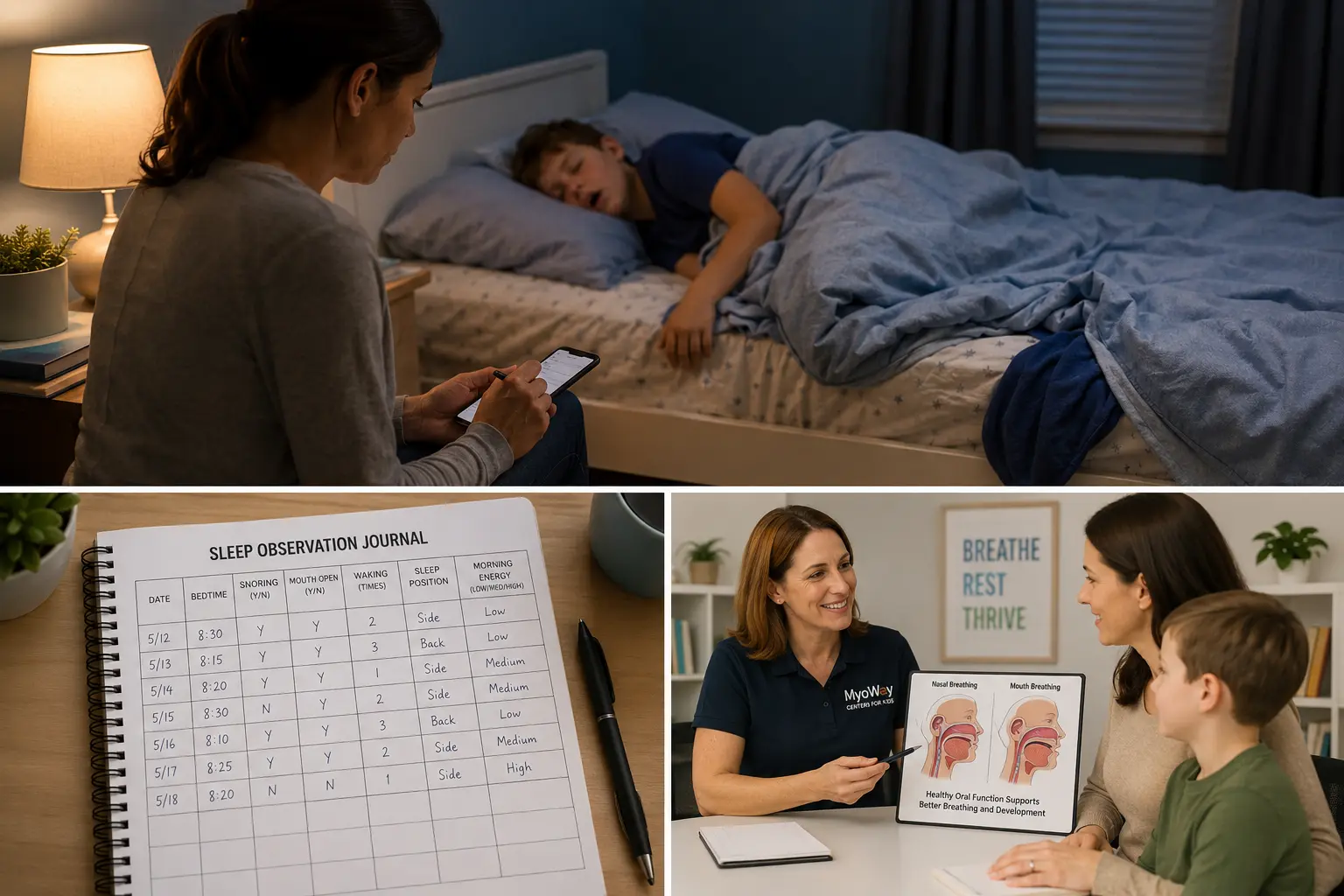
Parents usually know when their child is not sleeping well. They hear snoring from the hallway, notice blankets on the floor, or find their child sleeping in an unusual position with an open mouth. By morning, that same child may be difficult to wake, unusually emotional, unfocused, or exhausted.
Then a sleep study comes back normal, borderline, or unclear.
That result can leave families wondering what to do next. Were the symptoms unimportant? Did the test miss something? Should they simply wait and see?
A pediatric sleep study can provide valuable medical information. However, it represents only one part of the overall picture. What parents observe over many nights can also help providers understand how a child breathes, sleeps, and functions during the day.
The goal is not to choose between a sleep test and a parent’s observations. Both can provide useful information and deserve careful consideration.
What a Pediatric Sleep Study Measures
An overnight sleep study, also known as polysomnography, records several body functions while a child sleeps. Depending on the study, it may measure airflow, breathing effort, oxygen levels, heart rate, brain activity, sleep stages, and body movement.
This testing plays an important role in identifying pediatric obstructive sleep apnea and other sleep-related concerns. Parent observations cannot measure oxygen levels or show how often breathing interruptions occur. For that reason, a home video, questionnaire, dental examination, or myofunctional evaluation should not replace a medically recommended sleep study.
At the same time, a sleep study answers specific diagnostic questions. It may not explain every reason a child snores, sleeps with an open mouth, moves constantly, or wakes feeling tired.
A result that does not confirm sleep apnea does not always mean every symptom lacks importance. Instead, it may signal the need for a broader conversation with the provider who ordered the study.
Why the Test May Not Match What Parents See
A sleep study usually records one night. That night can provide meaningful data, but it may not reflect a typical night at home.
A child may sleep in a different position or spend less time in certain sleep stages. The unfamiliar environment and monitoring equipment may also change how the child sleeps. Congestion, allergies, illness, medication, exhaustion, and sleeping position can cause symptoms to vary from night to night.
This does not make the test inaccurate. It means providers should interpret the results alongside the child’s health history and the patterns parents observe over time.
Not every sleep concern points to obstructive sleep apnea. Snoring and restless sleep may relate to nasal obstruction, enlarged tonsils or adenoids, allergies, asthma, oral breathing habits, insufficient sleep, anxiety, reflux, movement-related sleep concerns, or other medical issues.
Some children snore without meeting the criteria for sleep apnea. Providers sometimes call this primary snoring. It differs from obstructive sleep apnea, but frequent snoring and ongoing sleep disruption still deserve attention.
The American Academy of Pediatric Dentistry identifies snoring, mouth breathing, restless sleep, unusual sleeping positions, attention concerns, and witnessed breathing pauses as possible signs of pediatric sleep concerns. Parents can read the organization’s policy on obstructive sleep apnea in children for more information.
Why Parent Observations Matter
Parents see their children across weeks, months, and seasons. They notice patterns that may not appear during one appointment or one night of testing.
A parent may notice that a child snores most nights, sleeps with the neck tilted backward, wakes several times, sweats heavily, or seems exhausted every morning. These observations do not establish a diagnosis. However, they can help the healthcare team understand what happens at home.
Specific details are more useful than general descriptions. Instead of saying, “My child sleeps badly,” a parent might explain:
“My child snores four or five nights each week.”
“She usually sleeps with her mouth open.”
“He moves constantly and often ends up sideways in the bed.”
“She is difficult to wake and seems tired through most of the morning.”
“He struggles to focus during the day after a restless night.”
These details give providers a clearer view of how often symptoms occur and how much they affect the child.
Research suggests that parents may not mention sleep-related breathing symptoms during routine medical appointments unless someone asks directly. A study on which pediatric sleep-related breathing symptoms parents report during consultations found that structured questions can help bring important concerns into the discussion.
Signs to Pay Attention to at Night
Occasional restless sleep can happen for many reasons. A child may be sick, overtired, congested, or adjusting to a change in routine. Concern grows when symptoms happen often or appear with daytime difficulties.
Nighttime signs worth discussing with a healthcare provider include frequent snoring, mouth-open sleeping, noisy breathing, sweating, teeth grinding, repeated waking, unusual sleeping positions, or constant movement.
Some parents also notice that a child sleeps with the neck extended, wakes with a dry mouth, or seems to work harder than expected to breathe.
Witnessed pauses in breathing, gasping, choking, bluish coloring, or significant breathing effort require prompt attention. A child in acute distress needs medical care rather than a routine dental or myofunctional appointment.
Daytime Behavior Can Provide Additional Clues
Children do not always respond to poor sleep the same way adults do. An exhausted adult may look sleepy and quiet. A tired child may become restless, emotional, impulsive, or unusually active.
Some children struggle to wake up, complain of morning headaches, or seem foggy during breakfast. Others have trouble remembering instructions, staying focused in class, regulating emotions, or completing schoolwork.
These behaviors can have many causes. Sleep and breathing make up only part of the picture, so parents should not assume that every attention or behavior concern involves the airway.
Still, sleep deserves consideration when daytime concerns appear with snoring, mouth breathing, restless sleep, or difficult mornings. MyoWay’s article on how breathing can affect a child’s academic performance explains why nighttime breathing patterns may matter when families investigate focus and learning difficulties.
A study of five-year-old children also found links between parent-reported sleep-related breathing symptoms and hyperactivity, inattention, daytime sleepiness, and other behavioral findings. An association does not prove that breathing caused each problem. However, it supports asking about sleep when these patterns appear together. Parents can review the study Symptoms of Sleep-Disordered Breathing in 5-Year-Old Children.
What Parents Can Do Next
When a sleep study is normal, borderline, or unclear but symptoms continue, start with the provider who ordered or interpreted the test.
Ask what the result does and does not rule out. It may also help to ask whether the child slept long enough for the study to provide useful information. Parents can also ask whether the child reached the expected sleep stages and slept in a typical position.
Another useful question is whether the study showed snoring, airflow changes, repeated arousals, or oxygen changes that did not meet the threshold for a specific diagnosis.
Depending on the child’s symptoms, the next step may involve a pediatric sleep specialist, pediatrician, ear, nose, and throat specialist, allergist, dentist, orthodontist, or another healthcare provider.
A short sleep record can make the follow-up conversation more useful. For one or two weeks, parents can document bedtime, waking time, snoring, mouth-open sleep, restlessness, waking episodes, sleeping position, and morning behavior.
Short audio or video recordings may also help a physician understand what parents see or hear. Record them safely and respectfully. These recordings cannot replace formal testing, but they may show a pattern that did not occur during the study.
Looking Beyond the Sleep Study
After major medical concerns have been addressed, some children may benefit from an evaluation of breathing habits, oral function, tongue posture, and jaw development.
A pediatric myofunctional evaluation may examine whether a child breathes comfortably through the nose, keeps the lips closed at rest, positions the tongue well, and coordinates chewing and swallowing effectively.
The evaluation may also consider jaw and palate development, oral habits, and the symptoms parents notice at home.
This type of assessment does not diagnose obstructive sleep apnea. It also does not replace care from a pediatrician, sleep physician, or ear, nose, and throat specialist. Instead, it can add useful information about how the lips, tongue, jaw, and breathing patterns work together.
Families who are new to this area can learn more in Pediatric Myofunctional Therapy: More Than Just Mouth Exercises.
MyoWay’s Programs and Therapy page also explains how care may include oral muscle training, breathing education, home exercises, appliance guidance, and collaboration with other healthcare providers.
How Myofunctional Therapy Fits Into Care
Myofunctional therapy focuses on oral function. It may support nasal breathing habits, lip closure, tongue posture, swallowing coordination, and healthier oral muscle patterns.
It does not remove enlarged tonsils or adenoids. It also does not replace allergy treatment, medical management, orthodontic care, surgery, or another medically indicated treatment.
For some children, myofunctional therapy may become one part of a larger care plan. A pediatrician or sleep physician may guide diagnosis. An ear, nose, and throat specialist may evaluate the airway. An allergist may address ongoing nasal symptoms, while a dentist or orthodontist assesses the developing jaws and dental arches.
A myofunctional provider can focus on breathing habits, oral rest posture, muscle coordination, and swallowing patterns when those concerns are present.
The right approach depends on the individual child. An evaluation can help determine whether myofunctional therapy may be appropriate or whether another referral should happen first.
Questions Parents Often Ask
Can a child still have sleep problems after a normal sleep study?
Yes. A normal result may mean the child did not meet the criteria for the condition being tested, such as obstructive sleep apnea. Other factors may still affect sleep. These can include allergies, nasal obstruction, oral breathing habits, insufficient sleep, movement-related concerns, or another medical issue.
Are parent observations more important than a sleep study?
They provide different types of information. A sleep study measures breathing and sleep signals during the recorded night. Parents observe patterns over time. Both can be valuable, but parent observations alone cannot diagnose sleep apnea.
Is occasional snoring normal in children?
Temporary snoring may occur during a cold or a brief period of congestion. Frequent snoring should be discussed with a healthcare provider, especially when it occurs with restless sleep, mouth breathing, gasping, unusual sleep positions, or daytime concerns.
Can myofunctional therapy diagnose sleep apnea?
No. Myofunctional therapy does not diagnose sleep apnea. It evaluates oral muscle function, tongue posture, breathing habits, swallowing, and related developmental patterns.
Can myofunctional therapy help if the sleep study was normal?
It may help some children who have functional concerns such as habitual mouth breathing, poor lip closure, low tongue posture, or swallowing difficulties. An evaluation can help determine whether therapy is appropriate.
When should parents seek urgent medical care?
Parents should seek prompt medical care when a child has significant breathing difficulty, prolonged pauses, bluish or gray coloring, severe chest retractions, loss of consciousness, or another sign of acute distress.
Getting a Clearer Picture
Parents do not need to interpret sleep data or determine a diagnosis on their own. Their role is to notice patterns, document them clearly, and keep asking questions when a child does not seem rested or comfortable.
A sleep study can provide important objective information. Parent observations add context across many nights. A physical and functional evaluation may add another part of the picture.
Together, these perspectives can help families and healthcare providers make more informed decisions about what the child may need next.
MyoWay Centers for Kids offers brief, noninvasive evaluations focused on breathing patterns, tongue posture, oral function, jaw development, and the concerns families observe at home. Parents can learn more about the conditions evaluated at MyoWay or schedule a free consultation.
An evaluation does not provide a diagnosis or guarantee treatment results. It offers an opportunity to gather more information and decide whether myofunctional support, medical referral, or collaborative care may be appropriate.



